
A Laboratory Information Management System (LIMS) is defined as software that manages sample tracking, laboratory workflows, and quality control data. An Electronic Health Record (EHR) is defined as a digital system that stores patient medical histories, clinical encounters, and diagnostic results. Understanding the LIMS vs EHR explained distinction matters because confusing the two leads to costly procurement mistakes, integration failures, and compliance gaps. Both systems are essential in modern healthcare, but they serve fundamentally different masters: the sample and the patient, respectively.
What are the core differences in LIMS vs EHR explained?
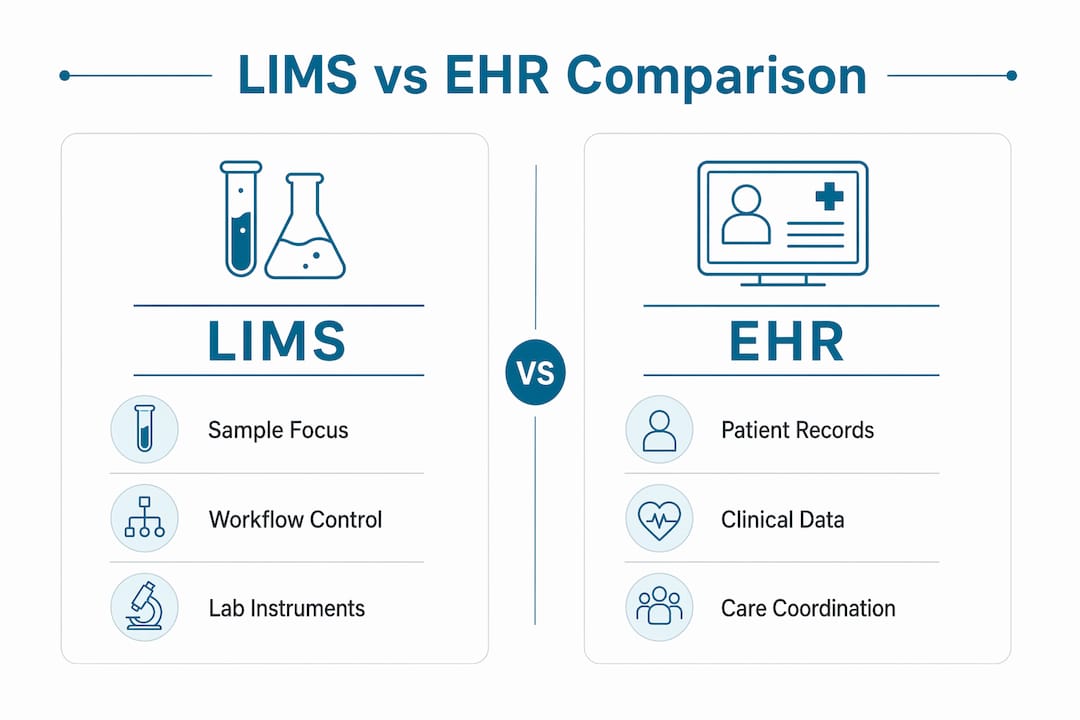
LIMS and EHR systems organize data around entirely different primary entities. A LIMS centers on the sample or batch. An EHR centers on the patient. That single distinction drives every architectural, workflow, and regulatory difference between the two systems.
A LIMS tracks a sample from collection through processing, analysis, and result generation. It manages instrument connections, reagent lot numbers, chain of custody, and quality control runs. Clinical labs use LIMS for research, manufacturing, and specialty diagnostics that require batch tracking and production-level traceability. Regulatory frameworks like GMP (Good Manufacturing Practice) and GLP (Good Laboratory Practice) govern LIMS environments in regulated industries.

An EHR manages the longitudinal patient record. It captures clinical encounters, physician orders, medication histories, diagnostic results, and billing codes. HIPAA and CLIA set the compliance baseline for EHR systems in U.S. clinical settings. EHR data flows between providers, payers, and patients across the care continuum.
The table below summarizes the core differences:
| Category | LIMS | EHR |
|---|---|---|
| Primary data entity | Sample or batch | Patient encounter |
| Core workflow | Sample intake, processing, QC, reporting | Clinical orders, diagnoses, prescriptions |
| Regulatory framework | GMP, GLP, ISO 17025 | HIPAA, CLIA, HL7 |
| Typical users | Lab scientists, QC managers, lab directors | Physicians, nurses, care coordinators |
| Integration target | Lab instruments, LIMS modules, LIS | Pharmacy, billing, imaging, lab results |
Pro Tip: If your primary question is "Where is this sample?" your team needs a LIMS. If your primary question is "What happened to this patient?" your team needs an EHR. The right system choice depends on which data entity drives your daily decisions.
How do LIMS and EHR systems integrate, and what challenges arise?
Integration between LIMS and EHR is the point where most healthcare organizations underestimate both the complexity and the ongoing cost. The typical workflow runs in one direction: a physician places an order in the EHR, the LIMS receives that order, manages the sample, and sends results back to the EHR for clinical review. That loop sounds simple. In practice, it breaks in predictable and expensive ways.
The most common failure point is patient identity. Duplicate Medical Record Numbers occur when patient identifiers diverge between the LIMS and EHR, creating direct patient safety risks. A sample linked to the wrong patient record can trigger incorrect treatment decisions. This is not a theoretical risk. It is a documented operational hazard in labs that rely on manual reconciliation or loosely configured interfaces.
Beyond identity mismatches, the following integration challenges affect nearly every organization running both systems:
- Version drift: Updates to either the LIMS or EHR can silently break existing interfaces. Ongoing maintenance costs frequently exceed initial implementation fees because each software update requires interface retesting and often reconfiguration.
- Data duplication: Without a clear system of record for each data type, the same result can exist in multiple places with conflicting values.
- Interface maintenance labor: Each HL7 or FHIR interface requires dedicated FTE hours for monitoring, troubleshooting, and updating. That cost rarely appears in initial vendor quotes.
- Disconnected stacks: Disconnected systems increase lab errors, cause reporting delays, and create revenue leakage through missed charges and manual re-entry.
Healthcare organizations consistently underestimate the resources required for sustained EHR and LIMS integration beyond the initial software purchase. The real cost is not the license fee. It is the ongoing engineering time, interface monitoring, and staff hours spent reconciling data that should have flowed automatically.
The most effective mitigation is defining clear domain ownership before go-live. The LIMS owns sample data. The EHR owns patient encounter data. Every interface should enforce that boundary rather than blur it.
When should you choose LIMS, EHR, or both?
The choice between systems depends entirely on whether the primary data entity is a patient or a sample, not on feature checklists. That principle cuts through most vendor confusion quickly.
Use these decision criteria to guide your selection:
-
Choose an EHR-centric approach when your organization's primary function is clinical care delivery. Hospital systems, outpatient clinics, and physician practices need EHR as the system of record. Lab results flow into the EHR as one data type among many.
-
Choose a LIMS-centric approach when your organization's primary function is laboratory production. Research labs, reference labs, genetic testing labs, and manufacturing quality labs need LIMS as the operational core. Patient identity is secondary to sample traceability.
-
Run both with clear boundaries when your organization operates in a hybrid environment. A hospital reference lab, for example, serves both clinical patients and research protocols. Running both systems concurrently with defined system-of-record boundaries preserves data integrity and operational efficiency.
-
Prioritize interoperability standards regardless of which system leads. HL7 v2, FHIR R4, and standardized patient identifiers like MPI (Master Patient Index) reduce integration failures before they start.
-
Assess regulatory obligations first. A pharmacogenomics lab operating under CLIA and CAP accreditation has different compliance requirements than a GMP manufacturing lab. The regulatory framework shapes which system must carry the audit trail.
Pro Tip: Before issuing any RFP, map your actual daily workflow on a whiteboard. Identify whether samples or patients appear first in every major process. That map will tell you which system should be primary before any vendor conversation begins. For genetic testing labs, the LIMS vs LIS decision adds another layer worth understanding.
What benefits does a modern LIMS bring to healthcare labs?
A well-implemented LIMS delivers measurable operational improvements that EHR systems are not designed to provide. Labs that properly integrate LIMS reduce processing and turnaround times by 30–40% compared to manual workflows. That reduction translates directly into faster patient results and lower labor costs per test.
The operational benefits of a modern LIMS in healthcare settings include:
- Reduced manual errors: Automated sample tracking eliminates transcription errors that occur when staff manually enter sample IDs, test codes, or result values.
- Real-time data sharing: Modern LIMS platforms integrate with hospital EHRs to enable real-time data flow, reducing duplication and improving care coordination.
- Compliance support: LIMS supports regulatory compliance through audit trails, quality control records, and full traceability, which are requirements under GMP and ISO 17025 standards.
- Instrument connectivity: A LIMS connects directly to analyzers, sequencers, and other lab instruments, pulling results automatically rather than requiring manual transcription.
- Workflow visibility: Lab managers gain real-time queue visibility, bottleneck detection, and turnaround time reporting without building custom reports in spreadsheets.
For genetic testing and molecular diagnostic labs specifically, LIMS benefits extend further. Sample chain of custody, accessioning, PGx report generation, and provider result delivery all require a workflow engine that EHR systems do not provide. A well-designed lab workflow built on a purpose-built LIMS reduces the manual handoffs that create errors and delays in high-volume specialty labs.
Key Takeaways
LIMS and EHR are complementary systems with distinct domains: LIMS owns sample data, and EHR owns patient encounter data. Confusing or conflating them creates integration failures, compliance gaps, and patient safety risks.
| Point | Details |
|---|---|
| LIMS is sample-centric | LIMS manages samples, batches, instruments, and QC data, not patient records. |
| EHR is patient-centric | EHR stores clinical encounters, diagnoses, and longitudinal health histories. |
| Integration costs are ongoing | Maintenance fees and version drift regularly exceed initial implementation costs. |
| Domain ownership prevents errors | Assigning each data type to one system of record reduces duplicate MRNs and data conflicts. |
| LIMS drives lab efficiency | Labs using LIMS report 30–40% faster processing times compared to manual workflows. |
Why the "just use the EHR" instinct costs labs more than they expect
Labs that default to using their EHR for sample management because "it's already there" pay for that decision in ways that rarely show up in the original budget conversation. I have seen this pattern repeatedly in molecular and genetic testing environments. The EHR handles the order and the result, so the assumption is that it handles everything in between. It does not.
The middle of the workflow, where samples are accessioned, tracked, processed, and validated, is exactly where EHR systems have no native capability. Labs fill that gap with spreadsheets, shared drives, and informal tracking systems. Those workarounds create the audit trail gaps, turnaround time problems, and compliance risks that regulators find during inspections.
The harder truth is that integration is not a one-time project. Version drift is real, and every major EHR or LIMS update is a potential interface failure waiting to happen. Labs that treat integration as a solved problem after go-live are the ones that get caught off guard six months later when a software update breaks their results interface.
My advice: treat LIMS and EHR as permanent co-owners of different data domains, and budget for the ongoing engineering work that keeps them synchronized. The labs that do this well are the ones that scale without operational chaos. The role of LIMS in lab compliance is not optional for regulated environments. It is the foundation.
— Tarek
How Labrynix supports LIMS and EHR integration for molecular labs
Labrynix is built specifically for genetic testing, molecular diagnostics, and pharmacogenomics laboratories that need more than a generic lab software platform.
The Labrynix LIMS platform manages the complete sample-to-report workflow, including order intake, accessioning, sample tracking, workflow queues, audit logs, and role-based access controls. Labrynix Connect supports HL7, FHIR, API, and webhook integrations with EHR systems, billing platforms, and lab instruments, giving labs a defined integration layer rather than a patchwork of point-to-point connections. Labrynix Intelligence adds AI-powered workflow automation, bottleneck detection, and operational analytics. For labs managing PGx reporting alongside clinical data, Labrynix brings LIMS, reporting, portals, and EHR integration into one connected system built around real molecular lab workflows.
FAQ
What is the main difference between LIMS and EHR?
A LIMS manages sample tracking, laboratory workflows, and quality control data. An EHR manages patient medical records, clinical encounters, and diagnostic histories. The core difference is the primary data entity: sample versus patient.
Can a LIMS replace an EHR in a clinical setting?
A LIMS cannot replace an EHR for clinical care delivery. LIMS handles sample and lab workflow data, while EHR handles patient records, physician orders, and care coordination. Clinical settings require both systems with clear integration boundaries.
Why does LIMS and EHR integration fail so often?
Integration failures most commonly result from version drift, duplicate patient identifiers, and underestimated maintenance costs. Ongoing interface maintenance frequently exceeds initial implementation fees as software updates break existing connections.
What compliance standards apply to LIMS versus EHR?
LIMS environments are governed by GMP, GLP, and ISO 17025 standards in regulated labs. EHR systems in U.S. clinical settings operate under HIPAA and CLIA requirements. Both systems require audit trails, but the specific regulatory frameworks differ significantly.
When does a lab need both LIMS and EHR?
A lab needs both systems when it operates in a hybrid clinical and research environment, such as a hospital reference lab or a genetic testing lab serving both patients and research protocols. Running both concurrently with defined system-of-record boundaries is the recommended approach.