
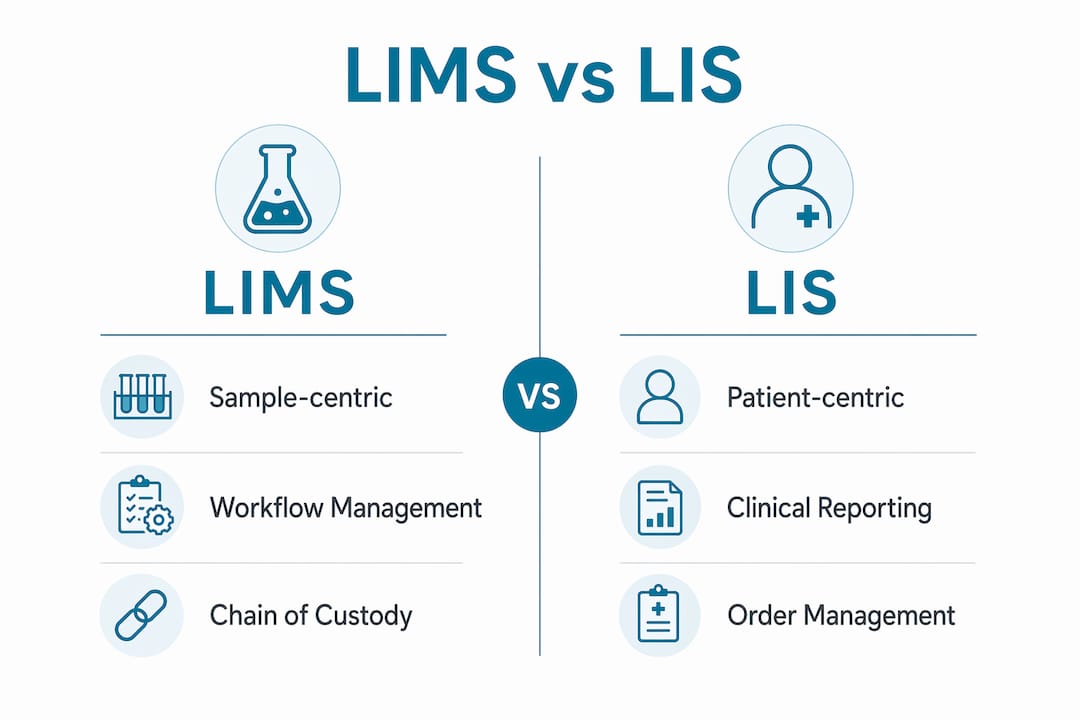
A LIMS (Laboratory Information Management System) is defined as a sample-centric platform that manages workflows, chain-of-custody, and quality control, while a LIS (Laboratory Information System) is a patient-centric platform that manages diagnostic orders, clinical results, and healthcare reporting. Understanding the LIMS vs LIS genetic testing distinction is not academic. It determines which system your lab can actually build a compliant, scalable workflow around. The core difference is that LIS focuses on diagnostic results tied to a patient, while LIMS focuses on the sample and what happens to it from accessioning through final disposition. Genetic testing labs, molecular diagnostic programs, and pharmacogenomics operations sit at the intersection of both worlds, which is exactly why this decision is harder than it looks.
What are the core functional differences between LIMS and LIS in genetic testing?
The design philosophy of each system shapes every feature it offers. LIMS tracks a sample through every step of its lifecycle: receipt, accessioning, storage, testing, QC review, and archival. LIS tracks a patient through every step of their diagnostic encounter: order entry, specimen collection, result reporting, and clinical communication.
In a molecular diagnostics lab, these two orientations produce very different workflows. A LIMS records that sample ID 2024-09-4471 was received, extracted, run on a sequencer, passed QC, and flagged for review. A LIS records that patient Jane Doe had a BRCA1 panel ordered by Dr. Smith, the specimen was collected, the result was negative, and the report was sent to her EHR. Both records matter. They describe the same event from different angles.

| Function | LIMS | LIS |
|---|---|---|
| Primary data object | Sample / specimen | Patient / order |
| Workflow focus | Sample lifecycle and QC | Diagnostic order and result |
| Instrument integration | Direct, bidirectional | Often via middleware |
| Reporting output | Batch reports, QC summaries | Clinical result reports, HL7 messages |
| EHR/EMR integration | Limited or via middleware | Native, deep integration |
| Regulatory framework | 21 CFR Part 11, ISO 17025 | HIPAA, CLIA, HL7 standards |
LIMS manages samples through workflow steps with audit trails and quality control, which is critical for manufacturing and research environments. That audit trail capability is what makes LIMS the preferred choice for regulatory submissions in genetic labs. LIS, by contrast, integrates deeply with clinical systems in ways LIMS was never designed to do, including native HL7 messaging, patient privacy controls, and clinical decision support.
Pro Tip: Map your lab's primary data object before evaluating any system. If your team asks "where is this sample?" more than "what happened with this patient?", your core need is LIMS, not LIS.
What are the advantages and disadvantages of LIMS in genetic testing workflows?
A well-implemented LIMS delivers measurable returns. Operational efficiency gains from LIMS typically produce ROI within one year, driven by reduced paperwork and automated instrument interfacing. For a genetic testing lab processing hundreds of samples per day, that automation compounds quickly across accessioning, extraction, sequencing, and QC steps.
LIMS also delivers sample traceability, chain-of-custody, and batch management that are required for regulatory submissions in genetic labs. Without these capabilities, labs face manual tracking, spreadsheet errors, and audit failures. LIMS eliminates those risks by enforcing structured data entry at every workflow step.
The disadvantages are real and worth planning for:
- Scope creep. LIMS projects frequently suffer from scope creep, requiring clear project goals to avoid budget overruns. Labs that start with "let's also add billing tracking" mid-implementation routinely delay go-live by months.
- Bench-side documentation gaps. LIMS lacks the capability to capture real-time experimental observations at the bench, requiring supplemental tools. Scientists miss transient observations that never make it into the system.
- Data migration complexity. Integration complexity and legacy data migration are major challenges affecting LIMS ROI and project success. Inconsistent sample IDs and free-text fields discovered late in the process make fixes expensive.
- User adoption failures. Poor user adoption and irregular process documentation cause high data quality degradation after implementation. The system is only as good as what staff actually enter into it.
Pro Tip: Audit your existing sample ID conventions and data entry fields before any LIMS configuration begins. Inconsistencies found after configuration starts cost significantly more to fix than those caught before the project kicks off.
When should a lab choose LIS versus LIMS for genetic testing?
Choosing between LIS and LIMS is fundamentally about the lab's primary mission: diagnostic patient care versus research or quality control workflows. That single question resolves most of the confusion.
Use this decision framework:
-
Choose LIS if your lab is a clinical diagnostic environment. LIS is essential in clinical diagnostic labs because it integrates with EHR and EMR systems and centers workflows around patient care and clinical reporting. Hospital-based genetic testing programs, hereditary cancer clinics, and reference labs sending results directly to physicians need LIS as their primary system.
-
Choose LIMS if your lab runs research, QC, or batch-heavy workflows. Pharmacogenomics labs processing large sample volumes, biobanks, and labs supporting regulatory submissions need LIMS. The sample tracking, batch management, and audit trail features are built for exactly this environment.
-
Choose a hybrid approach if your lab does both. Hybrid approaches combining LIS and LIMS are common in specialty genetic labs managing both clinical reporting and sample traceability. A PGx lab that reports results to physicians via HL7 while also managing complex extraction batches and QC workflows is a textbook hybrid candidate.
-
Evaluate integration requirements before committing. A LIMS without a clear path to EHR connectivity creates a reporting bottleneck for any lab delivering clinical results. Confirm that your chosen system supports HL7, FHIR, or API connections to the downstream systems your providers use.
-
Consider your regulatory submission obligations. Labs submitting data to the FDA or operating under CAP/CLIA accreditation need the audit trail and chain-of-custody features that LIMS provides natively. LIS systems handle HIPAA and clinical compliance well but were not designed for sample-level regulatory submissions.
The genetic testing LIS guide from Labrynix covers this decision in detail for labs that sit at the clinical and molecular intersection.
How do LIMS and LIS support compliance, data integrity, and reporting?
Compliance in genetic testing labs is not a single standard. It is a stack of overlapping requirements: HIPAA for patient data, CLIA for clinical testing, CAP for accreditation, and 21 CFR Part 11 for electronic records in FDA-regulated environments. LIMS and LIS address different layers of this stack.
LIMS compliance features center on sample data integrity:
- Audit trails recording every action taken on a sample record
- Electronic signatures for result approval and QC sign-off
- Chain-of-custody documentation from receipt through disposal
- Batch validation and instrument interface logs
LIS compliance features center on patient data protection and clinical accuracy:
- Patient privacy controls aligned with HIPAA requirements
- Clinical result validation workflows with physician notification
- HL7 message logs for EHR result delivery
- Order management tied to patient identity, not just specimen ID
Both systems require rigorous 21 CFR Part 11 validation, and post-configuration changes demand re-validation, which delays go-live milestones. This is one of the most underestimated costs in lab software projects. A configuration change made three weeks before launch can push the go-live date back by a month if IQ/OQ/PQ testing must be repeated.
The lab compliance standards guide from Herbilabs explains the full compliance framework for regulated research and genetic testing environments. For labs managing both sample traceability and patient privacy, the practical answer is a connected system where LIMS and LIS functions share a common data layer rather than operating as two separate silos.
Key Takeaways
LIMS and LIS serve different primary functions, and genetic testing labs that confuse the two end up with compliance gaps, reporting bottlenecks, or both.
| Point | Details |
|---|---|
| LIMS is sample-centric | LIMS tracks sample lifecycle, chain-of-custody, and batch QC from receipt through archival. |
| LIS is patient-centric | LIS manages diagnostic orders, clinical results, and EHR integration tied to patient identity. |
| Hybrid systems are common | Specialty genetic labs often need both systems connected to handle clinical reporting and sample traceability. |
| Compliance layers differ | LIMS addresses 21 CFR Part 11 and sample traceability; LIS addresses HIPAA and clinical result delivery. |
| Workflow audit before software | Optimizing internal processes before selecting a system prevents scope creep and data quality failures. |
What I've learned from watching labs pick the wrong system
Labs almost always underestimate how much their choice of LIMS versus LIS reflects their identity, not just their workflow. A lab that thinks of itself as a clinical service will gravitate toward LIS even when its actual daily operations are 80% sample management. That mismatch creates friction from day one.
The most consistent mistake I see is labs selecting software before they have mapped their own processes. Software automates existing processes and cannot fix broken ones. A LIMS installed on top of a chaotic accessioning workflow produces a faster, more expensive version of the same chaos. The labs that get the most out of their systems are the ones that spent two or three months cleaning up their process documentation before a vendor ever entered the room.
The bench-side documentation gap is the other issue nobody talks about honestly. Mobile data capture tools integrated with LIMS improve accuracy and compliance by capturing transient observations that scientists would otherwise lose. Most labs I've seen treat this as a nice-to-have. It is not. It is the difference between a LIMS that reflects reality and one that reflects what staff remembered to type in at the end of their shift.
My practical advice: if your lab delivers genetic results to physicians, you need LIS-grade clinical reporting and EHR connectivity. If your lab processes samples in batches with QC gates and regulatory submissions, you need LIMS-grade traceability. If you do both, build your architecture around a platform that connects the two rather than forcing a single system to do a job it was not designed for. The LIS/LIMS implementation timeline checklist is a good starting point for planning that architecture before you commit to a vendor.
— Tarek
How Labrynix supports genetic labs that need both LIMS and LIS capabilities
Genetic testing labs should not have to choose between sample traceability and clinical reporting quality. Labrynix was built specifically for labs that need both, combining LIMS workflow management, PGx reporting, provider and patient portals, HL7/FHIR integrations, and AI-powered insights in one connected platform.
Labrynix handles the complete sample-to-report workflow: order intake, accessioning, sample tracking, QC, pharmacogenomics report generation with CPIC guideline support and PharmGKB annotations, and secure result delivery to providers and patients. The platform supports HIPAA-conscious and GDPR-conscious operations with role-based access, audit logs, and configurable permissions. Labs managing complex genetic testing workflows can explore the full genetic testing lab software capabilities on the Labrynix platform, or review the flagship LIS/LIMS solution designed specifically for genetic and molecular labs.
FAQ
What is the main difference between LIMS and LIS?
LIMS is sample-centric, managing workflows, QC, and chain-of-custody for specimens. LIS is patient-centric, managing diagnostic orders, clinical results, and EHR integration.
What is LIS in genetics?
A LIS in genetics is a Laboratory Information System that connects genetic test orders to patient records, delivers results to EHR systems, and supports clinical reporting for physicians and patients.
Do genetic testing labs need both LIMS and LIS?
Many specialty genetic labs use hybrid approaches that combine LIMS sample traceability with LIS clinical reporting, especially when they serve both research and clinical diagnostic functions.
What are the biggest disadvantages of LIMS?
The most common LIMS disadvantages are scope creep during implementation, bench-side documentation gaps, legacy data migration complexity, and poor user adoption leading to data quality degradation.
How does 21 CFR Part 11 apply to LIMS and LIS?
Both LIMS and LIS require 21 CFR Part 11 validation for electronic records and signatures. Any post-configuration changes after validation require re-validation, which can delay deployment timelines significantly.