
A Laboratory Information Management System, or LIMS, is defined as software that manages laboratory samples, workflows, and associated patient data to support accurate, compliant lab operations. LIMS patient data management refers specifically to how that software captures, links, and tracks patient identifiers alongside sample records throughout the testing process. For laboratory professionals and healthcare administrators, understanding what LIMS does with patient data is not optional. It determines whether your lab can meet HIPAA, CLIA, and ISO 17025 requirements without manual workarounds. This guide breaks down the core functions, the critical differences from a Laboratory Information System (LIS), and the integration realities you need to know before selecting or configuring a system.
What is LIMS patient data management vs. LIS?
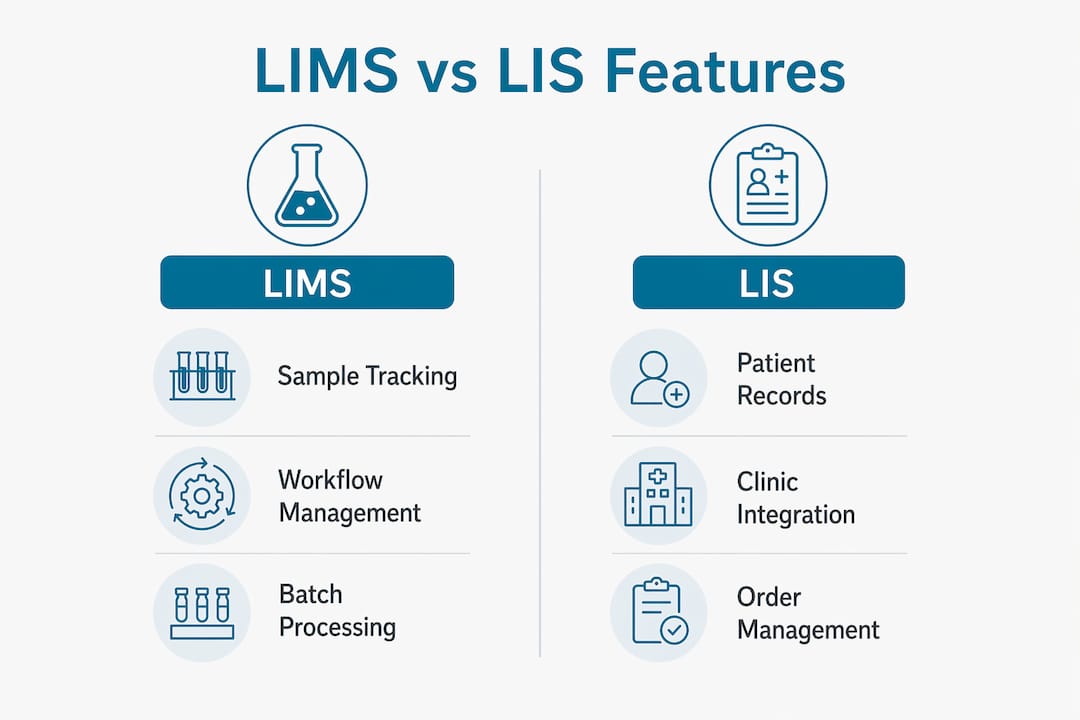
LIMS patient data management is sample-centric by design. The system organizes workflows around the sample itself, with patient identifiers attached as metadata rather than as the primary record. A Laboratory Information System, or LIS, takes the opposite approach. LIS is patient-centric, managing clinical orders, longitudinal patient records, and result delivery in ways that directly support clinical decision-making.
![]()
This distinction matters more than most labs realize. Choosing a sample-centric LIMS for a patient-centric diagnostic workflow creates gaps in clinical decision support tools that are vital for patient safety and compliance. A molecular diagnostics lab running pharmacogenomics panels, for example, needs patient medication history linked to results. A standard LIMS does not carry that context natively.
The table below shows where each system fits:
| Feature | LIMS | LIS |
|---|---|---|
| Primary focus | Sample and workflow tracking | Patient records and clinical orders |
| Patient data role | Linked metadata to samples | Core record structure |
| Typical use case | Research, molecular, PGx labs | Hospital and clinical diagnostic labs |
| Regulatory framework | GLP, GMP, ISO 17025/15189 | HIPAA, CLIA, CAP |
| Cost range | $25,000–$500,000+ | $50,000–$1,000,000+ |
| Clinical decision support | Limited | Built-in |
Clinical labs must comply with HIPAA, CLIA, and CAP, while research labs using LIMS primarily follow GLP, GMP, and ISO 17025/15189. That regulatory split explains why the two systems evolved differently and why swapping one for the other creates compliance risk.
Pro Tip: If your lab handles both research samples and clinical patient orders, you likely need both systems connected through an interface layer rather than one system trying to do both jobs.
What core features does LIMS use for patient data?
LIMS manages patient and sample data including assays, batch details, chain of custody, and instrument records for end-to-end laboratory workflow management. The patient data component is specific and bounded. Here is what a well-configured LIMS handles:
- Sample labeling and accession IDs linked to patient identifiers at intake, preserving traceability from collection through result
- Chain-of-custody tracking that records every handler, location change, and time stamp associated with a patient's sample
- Assay and batch management that ties test methods, reagent lots, and instrument runs back to the originating patient sample record
- Instrument integration that pulls raw data directly from analyzers into the LIMS record, eliminating manual transcription errors
- Audit trails that log every data entry, modification, and access event for regulatory review under GLP and ISO 15189
- Quality control records linked to patient sample batches, so a QC failure flags the associated patient results automatically
Typical patient data managed in LIMS includes sample IDs linked to patient identifiers, test metadata, and batch processing history. That linkage preserves traceability while keeping the workflow centered on samples rather than clinical records.
The practical implication is that LIMS gives you a complete forensic record of what happened to a sample. What it does not give you is a clinical narrative. For pharmacogenomics labs, this means the LIMS handles the sample side while a reporting layer, such as Labrynix Reports, handles the clinical interpretation and provider-facing output.
Pro Tip: Configure your LIMS to capture patient demographic fields at accession rather than importing them post-run. Retroactive data entry is the single largest source of patient ID errors in molecular labs.
How does LIMS integrate with EMR and EHR systems?
Interoperability is the most critical and challenging aspect of implementing LIMS in clinical environments due to complex data mapping requirements. Most labs discover this after go-live, not before. The core problem is structural. LIMS organizes data around sample IDs. EMR and EHR systems organize data around patient encounter records. Translating between those two structures requires careful field-level mapping, not just a generic HL7 connection.
EMR and EHR integration with LIMS requires careful HL7 message mapping, including handling order codes, specimen IDs, and result formats to avoid workflow interruptions. Here is how successful labs approach this:
- Audit your data fields before integration. Map every patient identifier, order code, and result field in your LIMS against the corresponding fields in your EMR. Mismatches at this stage are far cheaper to fix than post-integration.
- Use HL7 v2.x or FHIR R4 as your interface standard. HL7 v2.x remains the most widely supported in legacy hospital systems. FHIR R4 is the standard for modern API-based integrations and is required for many new EHR deployments.
- Test with real patient scenarios, not synthetic data. Synthetic test records rarely expose the edge cases, such as hyphenated names, duplicate MRNs, or split encounters, that break integrations in production.
- Build a reconciliation workflow. Even well-mapped integrations produce mismatches. A daily reconciliation report comparing LIMS sample records against EHR orders catches discrepancies before they affect patient care.
- Document every interface decision for compliance. HIPAA requires that you can demonstrate how patient data moves between systems. Your integration documentation is part of your compliance record.
Integration failures most often occur from differences in how orders and results are encoded across systems. A lab that uses local order codes in its LIMS but receives LOINC-coded orders from its EHR will break silently until a result fails to post. Platforms like Labrynix Connect are built to handle HL7, FHIR, APIs, and webhooks as native integration pathways, which reduces the custom development burden most labs face with generic LIMS products.
What best practices optimize lims-based patient data management?
Successful LIMS implementations require thorough staff training, validation, and compliance documentation to optimize patient data management and regulatory adherence. Common pitfalls include inadequate training and underestimating compliance complexity. The following practices separate labs that get full value from their LIMS from those that spend years managing workarounds.
Assess your workflow before selecting features. A PGx lab has different LIMS requirements than a high-throughput clinical chemistry lab. Map your sample volume, test menu, turnaround time targets, and reporting requirements before configuring any module. Generic configurations create friction at every step.
Train staff on patient data handling specifically. Most LIMS training focuses on sample tracking mechanics. Patient data handling, including how to correct a patient ID error, how to handle a duplicate accession, and when to escalate a data discrepancy, requires its own training track. Errors in patient identifiers are the most consequential errors a lab can make.
Validate every patient data workflow before go-live. Validation is not optional under ISO 15189 or CLIA. Document that your LIMS correctly links patient identifiers to sample records, correctly propagates those links through batch processing, and correctly exports them to downstream systems.
Manage hybrid LIS-LIMS environments deliberately. Many labs run both systems. The risk in a hybrid environment is data duplication and version conflicts, where the LIMS and LIS hold different values for the same patient field. Designate one system as the authoritative source for each data type and enforce that designation in your SOPs.
Audit your patient data linkages quarterly. Sample-to-patient linkage errors accumulate silently. A quarterly audit comparing LIMS patient IDs against source requisitions catches drift before it becomes a compliance finding.
For labs exploring LIMS workflow design in depth, the functional requirements differ significantly between molecular and clinical chemistry environments. Knowing those differences before configuration saves months of rework.
Key takeaways
LIMS patient data management is sample-centric by design, and labs that treat it as a patient record system create compliance gaps that are expensive to close.
| Point | Details |
|---|---|
| LIMS vs. LIS distinction | LIMS is sample-centric; LIS is patient-centric. Mixing them up creates clinical decision support gaps. |
| Core patient data features | LIMS links patient IDs to samples at accession and tracks chain of custody, assays, and audit trails. |
| Integration is the hardest part | HL7 and FHIR connections require field-level mapping; generic interfaces break silently on real patient data. |
| Compliance frameworks differ | LIMS follows GLP and ISO 17025/15189; clinical labs add HIPAA, CLIA, and CAP requirements. |
| Validation is non-negotiable | Every patient data workflow must be validated and documented before go-live under ISO 15189 and CLIA. |
Where LIMS patient data management is actually heading
The labs I see struggling most with patient data management are not the ones with bad software. They are the ones that bought a LIMS and expected it to behave like an LIS. That confusion is expensive. It shows up as manual workarounds, compliance findings, and result delivery delays that erode provider trust.
What I find genuinely interesting about the current moment is how molecular and PGx labs are forcing the industry to rethink the LIMS model. These labs need sample-centric workflow management and patient-centric reporting in the same operational cycle. A pharmacogenomics result is meaningless without the patient's medication list. That clinical context has to come from somewhere, and a traditional LIMS was never designed to carry it.
The labs getting this right are building connected architectures rather than looking for one system to do everything. They use a LIMS for what it does well, sample tracking, batch management, instrument integration, and audit trails, and they connect it to specialized reporting and portal tools that handle the patient-facing side. That separation of concerns is not a compromise. It is the correct architecture for precision medicine.
The compliance picture is also maturing. HIPAA-conscious design is no longer a differentiator. It is a baseline expectation. Labs that have not formalized their patient data governance, including role-based access, audit logs, and documented integration decisions, are carrying regulatory risk they may not have fully priced.
My honest advice: before you configure another LIMS module, draw the full data flow from patient requisition to result delivery and mark every point where patient identifiers move between systems. That map will tell you more about your compliance exposure than any vendor demo.
— Tarek
How Labrynix handles LIMS patient data management
Labrynix is built specifically for the labs where LIMS and patient-centric reporting have to work together in one workflow.
The Labrynix LIMS platform manages test orders, patient and provider information, accessioning, sample status, workflow queues, and audit activity in one connected system. Labrynix Connect handles HL7, FHIR, API, and webhook integrations so patient data moves cleanly between your LIMS and external EMR or EHR systems. Labrynix Reports adds AI-powered PGx reporting with CPIC guideline support and PharmGKB-informed annotations, giving your lab the patient-facing output that a standard LIMS cannot produce. For labs that need reporting dashboard visibility across sample and patient data, Labrynix brings those views into one operational interface.
FAQ
What is LIMS patient data management?
LIMS patient data management is the process by which a Laboratory Information Management System captures, links, and tracks patient identifiers alongside sample records throughout laboratory workflows. The system is sample-centric, meaning patient data serves as linked metadata rather than the primary record structure.
How is LIMS different from LIS for patient data?
A LIMS focuses on sample tracking, batch management, and lab workflows with patient data attached as metadata. An LIS is patient-centric, managing clinical orders, longitudinal patient records, and result delivery for direct clinical use.
What regulations apply to LIMS patient data in clinical labs?
Clinical labs using LIMS must address HIPAA, CLIA, and CAP requirements in addition to the GLP and ISO 17025/15189 standards that govern research LIMS environments. The regulatory framework depends on whether the lab performs clinical diagnostic testing or research-only work.
Why does LIMS and EMR integration fail so often?
Most integration failures occur from differences in how orders and results are encoded across systems, not from the absence of an HL7 interface. Field-level mapping mismatches between sample-centric LIMS records and patient-centric EHR records are the primary cause.
Do pgx labs need both a LIMS and an LIS?
Most pharmacogenomics labs need a LIMS for sample and workflow management plus a specialized reporting layer for patient-facing PGx results. A full clinical LIS is not always required, but the reporting and portal functions it provides must be covered by another system in the architecture.