
A Laboratory Information Management System (LIMS) serves as the centralized platform that connects test orders, clinical data, and billing processes to ensure accurate charge capture and reduce payment delays. The role of LIMS in lab billing coordination goes well beyond sample tracking. When LIMS and billing systems share data in real time, laboratories eliminate the manual handoffs that cause claim denials, revenue leakage, and compliance exposure. Standards like HL7 and FHIR make that connection possible. Platforms like Labrynix are built to make it practical for genetic and molecular labs operating at scale.
How does LIMS improve billing accuracy and prevent claim denials?
LIMS improves billing accuracy by automating charge capture directly from test orders, which removes the manual coding step where most errors originate. When a test order is entered, the LIMS generates a charge event tied to the correct procedure code, patient demographics, and ordering provider. That automation prevents missed charges and reduces the coding errors that trigger payer denials.

The more powerful mechanism is upstream validation. Embedding billing-aware rules such as medical necessity prompts and payer-specific edits directly inside LIMS workflows catches problems before a claim is ever submitted. A lab running pharmacogenomics panels, for example, can configure the LIMS to flag orders that lack required diagnosis codes at the point of order entry. The billing team never sees a defective order because the clinical workflow already corrected it.
Payer rules change frequently, and a LIMS that carries those rules upstream protects revenue in ways that post-submission scrubbing cannot. Consider these common denial triggers that upstream LIMS validation addresses:
- Missing or incorrect ICD-10 diagnosis codes at order entry
- Orders placed without required prior authorization flags
- Duplicate order submissions for the same patient and test within a payer-defined window
- Mismatched provider NPI numbers between the order and the claim
- Test panels billed without supporting medical necessity documentation
Pro Tip: Map your top five denial reason codes back to the specific LIMS data field that was missing or incorrect. That exercise almost always reveals a fixable gap in your order entry workflow rather than a billing department problem.
What technical standards enable LIMS and billing system integration?
The technical foundation of LIMS and billing integration rests on two messaging standards. HL7 v2.x is widely used for instrument and EMR connectivity, while FHIR supports newer API-based connections and patient portals. Interface engines sit between these systems and handle message transformation, routing, and error logging. Without an interface engine, a single format mismatch between the LIMS and a clearinghouse can silently drop charges.
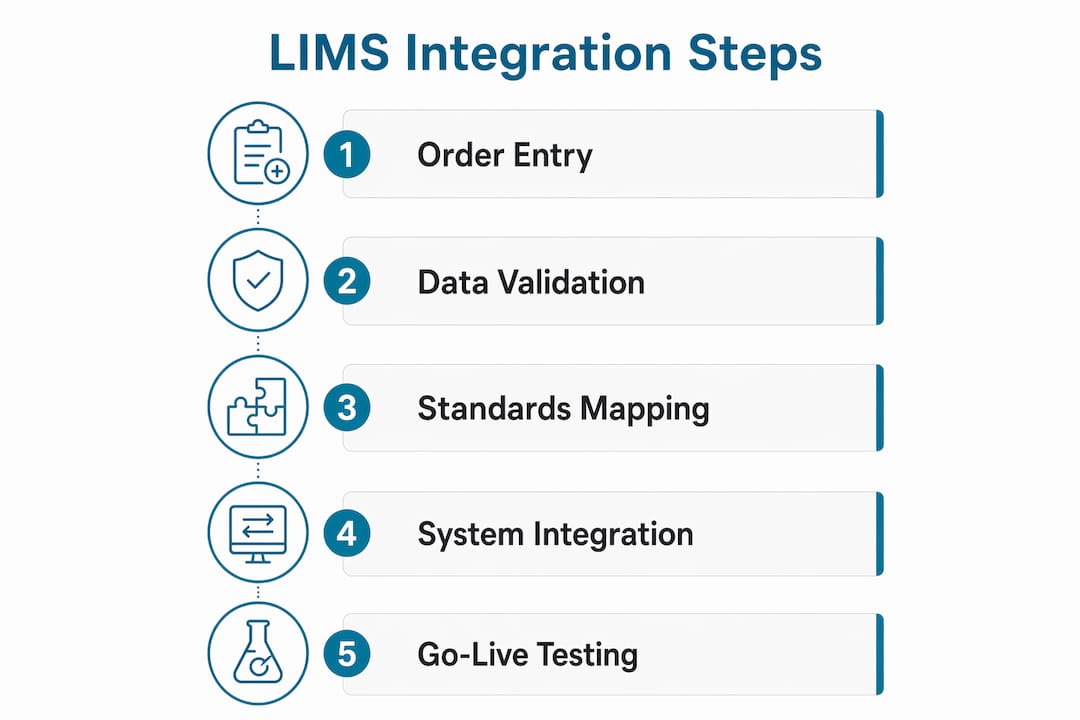
A typical LIMS-to-billing integration follows this sequence:
- Order entry triggers an HL7 ORM (order) message from the LIMS to the billing system.
- Result finalization sends an HL7 ORU (result) message that confirms the test was performed and supports medical necessity.
- Charge generation fires an automated charge event mapped to the correct CPT code and payer contract.
- Claim submission routes the formatted claim through a clearinghouse for eligibility and edit checks.
- Remittance posting returns ERA (electronic remittance advice) data to the LIMS billing module for reconciliation.
The table below summarizes the key standards and their roles in this workflow.
| Standard | Primary Use | Direction |
|---|---|---|
| HL7 v2.x | Order and result messaging | Bidirectional |
| FHIR R4 | API-based data exchange | Bidirectional |
| X12 837 | Claim submission to payers | Outbound |
| X12 835 | Remittance and payment posting | Inbound |
Integration go-live timelines typically range from 2–4 weeks for established systems that support HL7 and API interfaces. That timeline assumes clean data mapping and a cooperative clearinghouse. Labs with legacy systems or non-standard code sets should budget additional time for field-level mapping and testing.
Pro Tip: Before signing any integration contract, ask the vendor for a field-level mapping document. Vague interface specs are the single biggest cause of delayed go-live dates and post-launch billing errors.
What happens when LIMS and billing systems are not integrated?
Disconnected LIS and billing workflows cause denials because incomplete or inaccurate data reaches the billing system through manual re-entry. Staff copy patient demographics, diagnosis codes, and test identifiers from one screen to another. Each manual transfer is an opportunity for a keystroke error that becomes a denial weeks later.
The financial consequences compound quickly. Delayed payments stretch accounts receivable cycles. Repeated denials require rework that consumes billing staff time. Some charges are never recovered because the appeal window closes before the error is identified. Compliance risk rises when documentation gaps create audit exposure under Medicare or Medicaid billing rules.
"A well-integrated LIMS unifies clinical and financial workflows to scale lab operations efficiently. LIMS and billing systems do not function independently. Labs that treat them as separate tools pay for that separation in revenue leakage and operational drag."
The problems that siloed systems create fall into predictable categories:
- Data silos: Clinical staff and billing staff work from different records with no shared source of truth.
- Manual entry errors: Demographic mismatches between the LIMS and the billing system are the leading cause of eligibility denials.
- Revenue leakage: Tests performed but never billed because charge capture depends on a manual step that gets skipped.
- Compliance gaps: Missing result documentation that is required to support medical necessity on audit.
Siloed workflows between labs and billing drive revenue leakage that integration upstream in the lab workflow prevents. The fix is not a better billing team. The fix is a LIMS that carries billing logic into the clinical workflow from the first moment an order is placed.
How can lab managers optimize LIMS for better billing coordination?
Optimizing LIMS for billing coordination starts at test order entry, not at the billing department. Embedding billing logic such as payer-specific rules and medical necessity edits at the order level converts every order into a financial asset from the start. Labs that treat billing as a downstream function consistently underperform on clean claim rates compared to labs that build billing awareness into their LIMS workflows.
Ongoing interface management is equally critical. Each interface carries unique failure modes and mapping requirements that must be validated continuously as payer rules, code sets, and system versions change. A lab that validates its LIMS-to-clearinghouse interface once at go-live and never again will accumulate silent mapping errors over time. Assign a named owner to each interface and schedule quarterly validation reviews.
Practical steps for lab managers and billing coordinators include:
- Audit order entry workflows to confirm that required billing fields (diagnosis codes, ordering provider NPI, insurance information) are mandatory, not optional.
- Review test code management quarterly to catch CPT code updates, new payer edits, and panel bundling rules before they cause denials.
- Monitor interface logs daily for message failures, mapping errors, and acknowledgment timeouts that indicate a broken data feed.
- Cross-train clinical and billing staff on each other's workflows so that order entry staff understand why certain fields matter and billing staff can trace errors back to their source.
- Use lab billing ROI data to quantify the financial impact of denial rates and justify investment in interface upgrades or additional validation rules.
Pro Tip: Set up an automated alert for any day where the number of charge events generated by the LIMS is more than 5% below the number of finalized results. That gap is your missing revenue, and it shows up in real time rather than at month-end.
Key Takeaways
A LIMS that carries billing logic upstream into clinical workflows is the single most effective tool for reducing denials and protecting lab revenue.
| Point | Details |
|---|---|
| Upstream validation prevents denials | Embedding medical necessity and payer edits at order entry stops errors before claims are submitted. |
| HL7 and FHIR enable integration | These standards, managed by interface engines, connect LIMS to clearinghouses and billing platforms reliably. |
| Siloed systems cost real revenue | Manual re-entry between disconnected systems creates denials, leakage, and compliance exposure. |
| Integration is ongoing, not one-time | Interface validation and payer rule updates require continuous management after go-live. |
| Billing logic belongs in the LIMS | Treating billing as a downstream function consistently produces lower clean claim rates. |
Why I think labs underestimate what LIMS integration actually requires
Most labs I have worked with approach LIMS-to-billing integration as a technical project with a finish line. They go live, the charges flow, and the team moves on. That framing is the root cause of most billing performance problems I see six to twelve months later.
LIMS should be viewed as a continuous operational hub, not a one-time install. Payer rules change. CPT codes update every january. Clearinghouse mapping requirements shift when vendors release new versions. A lab that treats its interface as static will find that its clean claim rate quietly erodes while the team assumes everything is fine because charges are still flowing.
The other misunderstanding I see constantly is the belief that billing accuracy is the billing department's problem. The data that determines whether a claim pays or denies is created at order entry, not at claim submission. Putting payer logic inside the LIMS workflow is not a billing department request. It is a revenue protection decision that belongs at the lab director level.
Interface engine setup costs between $25,000 and $100,000 or more depending on the number of connected systems and the complexity of field-level mapping. That number surprises lab managers who expected a simple plug-in. It should not. The cost reflects the real complexity of making two systems agree on every data field for every transaction, every day, without errors. Labs that understand this upfront build better budgets and set more realistic timelines.
My recommendation is to assign a dedicated integration owner before go-live, not after the first billing problem surfaces. That person monitors interface logs, tracks payer rule changes, and owns the relationship between the LIMS team and the billing platform vendor. That role pays for itself within the first quarter.
— Tarek
Labrynix connects LIMS and billing for genetic and molecular labs
Labrynix is built for the labs where billing complexity is highest: genetic testing, molecular diagnostics, pharmacogenomics, and precision medicine. The platform connects LIMS workflow management with billing visibility, HL7 and FHIR integration pathways, and automated charge capture in one system designed around real lab operations.
Labrynix Billing gives lab managers and billing coordinators visibility into claim stages, invoice workflows, and revenue handoffs without switching between disconnected tools. Labrynix Connect supports HL7, FHIR, API, and webhook integrations with clearinghouses, EHR systems, and billing platforms. Labs exploring their options can review LIMS solutions by lab type to find the configuration that fits their specific workflow and billing coordination needs.
FAQ
What is the role of LIMS in lab billing coordination?
A LIMS centralizes test order data, patient demographics, and clinical results, then feeds that information directly to billing systems to automate charge capture and reduce manual errors. This connection is the foundation of accurate, timely claims submission.
How does LIMS integration reduce claim denials?
LIMS integration reduces denials by embedding payer-specific validation rules and medical necessity checks at order entry, catching missing or incorrect data before a claim is ever submitted to a clearinghouse.
What standards are used for LIMS and billing system integration?
HL7 v2.x handles order and result messaging, FHIR supports API-based data exchange, and X12 837/835 formats manage claim submission and remittance posting between LIMS platforms and billing systems.
How long does LIMS-to-billing integration take to implement?
Integration go-live timelines typically range from 2–4 weeks for systems that already support HL7 and API interfaces, though complex legacy environments or non-standard code sets can extend that timeline.
Why do labs lose revenue without integrated billing workflows?
Disconnected systems force manual re-entry of clinical data into billing platforms, which introduces demographic mismatches, missed charges, and documentation gaps that result in denials, delayed payments, and unrecovered revenue.